A guide for selecting the appropriate nasogastric tube
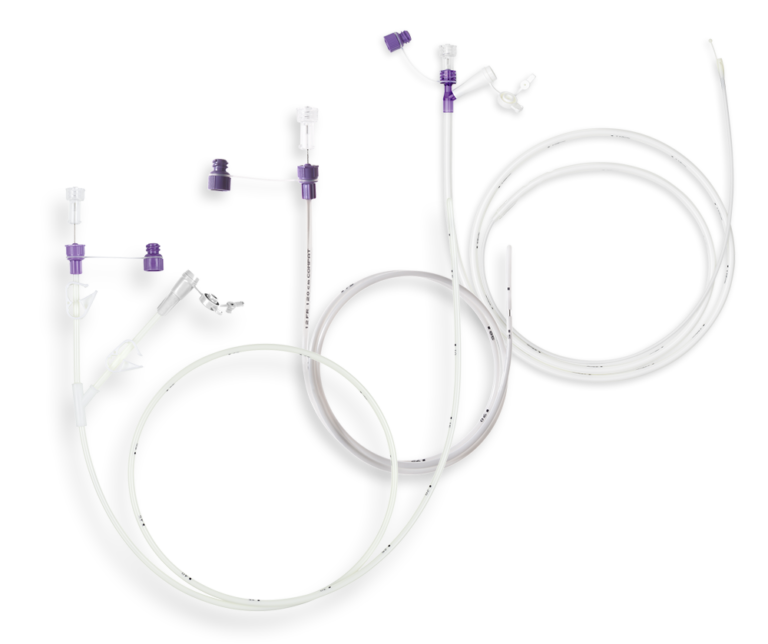
A nasogastric tube (NGT) is a flexible tube that is passed through the nose, down the oesophagus, and into the stomach. Generally used for enteral feeding and/or gastric drainage, NGTs offer a minimally invasive and usually well-tolerated solution by patients. However, they differ in their intended use, type of connector, material, size, and length. This article presents the key features of NGTs and provides guidance on NGT selection.
Intended use: enteral feeding or gastric drainage?
NGTs are used to provide enteral nutrition, water and medication directly into the patient’s stomach or small intestine.
NGTs can also be used for gastric drainage, which involves emptying all or part of the stomach contents. Gastric drainage alleviates bloating and symptoms associated with delayed gastric emptying as well as providing gastric secretions for diagnostic procedures1.
The intended use of an NGT influences a number of parameters, including the type of connector, number of lumens and tube material

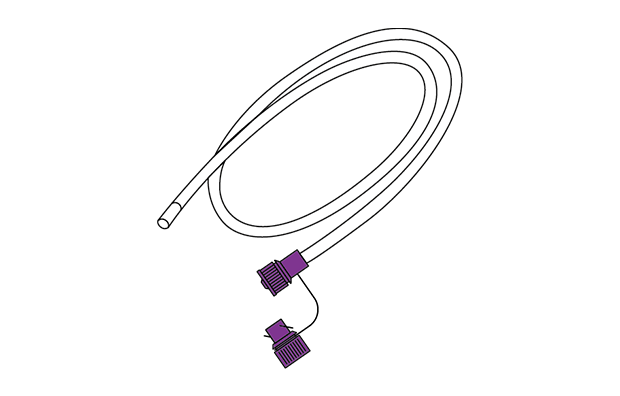
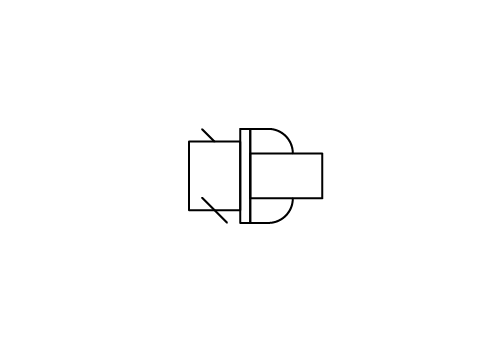
Drainage tube
Available as a single- or double-lumen NGT. Requires funnel connectors.
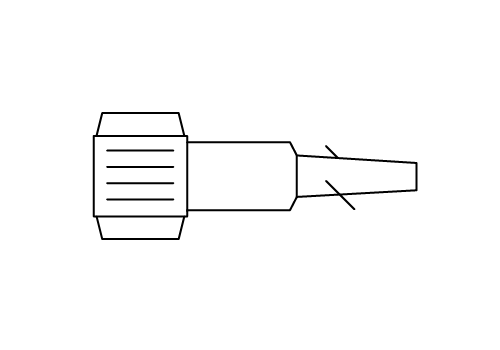
Feeding tube
Single-lumen NGT with ENFit connectors. Drainage is also possible with an ENFit syringe.
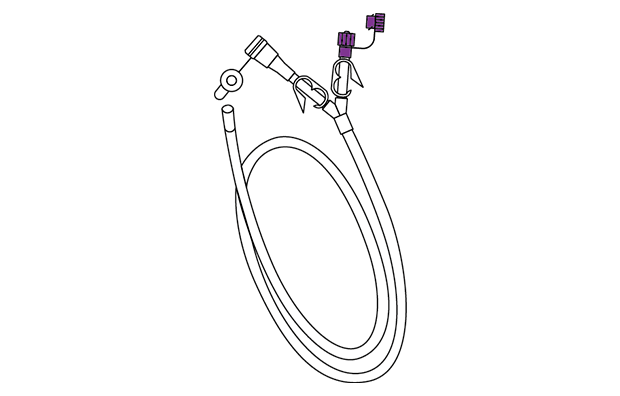
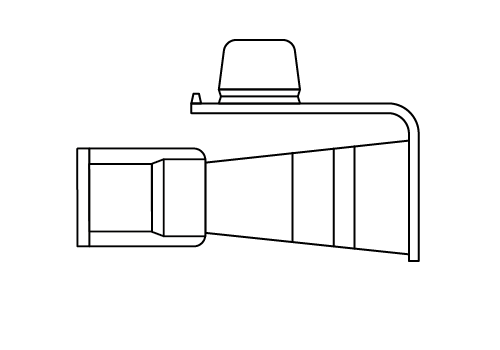
Feeding & drainage tube
Available with up to three lumens and multiple ports. Compatible with ENFit and funnel connectors to allow feeding and drainage through the same tube.
Tube Connectors: ENFit to promote patient safety
The connectors on the tube determine its compatibility with other medical devices such as with administration sets, syringes and accessories. These connectors, called small bore connectors, link and seal delivery systems together.
Patients may be connected to several delivery systems at once, such as an enteral feeding system, intravenous (IV) line, tracheostomy tube or peritoneal catheter. However, the legacy connectors are universal and compatible between one another, meaning that a medical device for one delivery system can be accidentally connected to a system designed for a different function. Such misconnections may put patients at risk and in some cases can be life-threatening. Given this risk, a global standard connector named ENFit was developed to promote safe and optimal delivery of enteral feeding.
 ENFit connectors are specifically designed for enteral feeding. They help to promote patient safety as they are incompatible with IV and other systems. This helps to prevent misconnections, which can have serious repercussions for patients2.
ENFit connectors are specifically designed for enteral feeding. They help to promote patient safety as they are incompatible with IV and other systems. This helps to prevent misconnections, which can have serious repercussions for patients2.
For more information, read the article ENFit: Promoting patient safety through a unique enteral-specific design.
Oral / Luer
The most widely used connector in multiple delivery systems. It allows different types of medical devices to be connected, thereby creating a risk of misconnection2.
Stepped and funnel type
Compatible with drainage or aspiration systems. Drainage tubes use a funnel connector which may also be compatible with the ENLock connectors prevalent in older enteral feeding tubes.
ENLock
The ENLock predates the ENFit industry standard. It is incompatible with IV systems but compatible with some drainage and aspiration connectors.
Tube diameter impacts patient comfort and clinical practices
The universal system for tube diameter is the French gauge (Fr), also known as the Charrière scale (Ch). The larger the Fr, the wider the external diameter of the tube. Each Fr increment equals 0.33 mm in diameter. NGTs typically range from 3.5 Fr3 for neonates to 14 Fr for adults and up to 24 Fr for triple-lumen gastric feeding/drainage tubes2.
Small-bore tubes (< 12 Fr) help to improve patient comfort and reduce the risk of tube feeding complications including rhinitis, oesophageal reflux, oesophagitis and oesophageal stricture. A small-bore tube should therefore be preferred where possible3.
It should also be noted that tubes between 8 Fr and 12 Fr are generally for feeding, whereas larger ones (> 12 Fr) are for drainage as their larger lumen is less likely to clog2.
Different materials for different indications
PVC, silicone and polyurethane are the most common materials for NGTs. This variety allows to meet a a range of indications, offering greater flexibility.
Polyvinyl Chloride
(PVC)
- This cost-effective, single-use material is commonly used for drainage tubes.
- Being stiffer, PVC is less likely to clog than softer, more malleable silicone or polyurethane2.
- Compared with other materials, PVC has lower biocompatibility4 and can stiffen over time, especially when exposed to gastric acid5.
- It is recommended for short-term use of up to 7 days*3
Silicone
(SIL)
- Soft, flexible and highly biocompatible3, silicone can be used for up to 6 weeks* with good patient comfort.
- Due to the pliable nature of silicone, there is an increased risk of kinking. Practitioners may find it helpful to use A stylet (guidewire) for tube insertion3.
Polyurethane
(PUR)
- A compromise in terms of cost and material rigidity.
- Softer than PVC but more rigid than silicone, polyurethane is a patient-friendly material that softens at body temperature6 for patient comfort.
- Highly biocompatible, it can be used for up to 6 weeks*3.
- Polyurethane tubes can have thinner walls than silicone ones, so their lumen can be larger even if their external diameter is the same.
- Some tubes are delivered with a stylet to ease insertion.
*In accordance with manufacturer specifications.
Tube length tailored to patient morphology and feeding site
NGTs are available in lengths of 90 to 165 cm for adults, or shorter for paediatric patients. Their length depends also on the tube’s placement site:
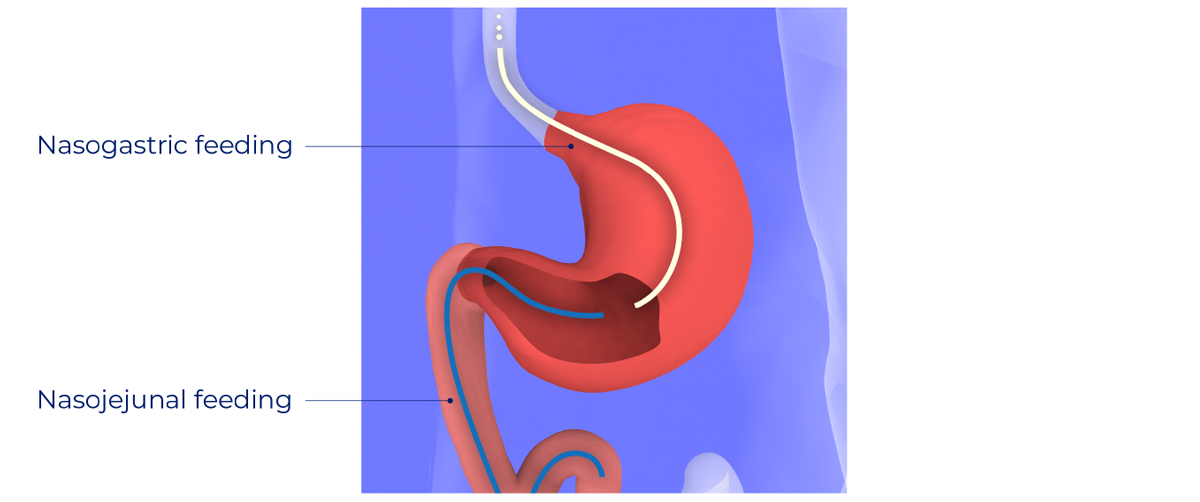
Gastric site:
- Nasogastric tubes are placed into the stomach for gastric feeding and/or drainage.
- Gastric access is appropriate in most cases, as it allows for more normal nutrient digestion.
- Gastric feeding tubes are typically between 90 and 120 cm long.
Jejunal site:
- Nasojejunal feeding tubes are placed into the small intestine, past the Ligament of Treitz2.
- Small intestine feeding access may be more suitable for patients with certain conditions including gastric outlet obstruction, gastroparesis, gastric fistula, pancreatitis, or risk of aspiration2.
- Jejunal feeding tubes are typically between 120 and 165 cm long.
Other features of NGTs
- Stylet: can be used to stiffen the tube and facilitate its placement into the patient as it reduces the risk of kinking. The stylet can be prelubricated to lower the risk of tube displacement on stylet removal. Use of stylets is subject to local regulations, and NGTs are therefore available with and without them.
- Radiographic visibility: NGTs can be completely radio-opaque or with radio-opaque markers to allow to verify their correct positioning on radiography3.
- Depth markings: tubes have depth markings to check placement depth and detect potential tube migration.
- Colour: Transparent NGTs allow practitioners to see the fluid flowing through the tube, making it easier to identify obstructions. However, such transparency must be weighed against carer/patient comfort, since they may prefer not to see the contents of the tube.
Risk of complications can be minimized with appropriate handling and care
NGT complications can be associated with tube insertion and tube care. The risk of complications can be minimised by employing appropriate preventative steps. Some of these include:
- Tube misplacement: Only trained staff should insert a tube and tube location should be confirmed according to local practices. Whenever possible, x-ray monitoring should be the favoured method.
- Tube migration or loss: Tubes should be secured and marked to allow position monitoring. Tube placement should be checked before each administration.
- Tube obstruction: Can be minimised by regular flushing with water as well as appropriate administration of medication.
- Aspiration: May be reduced by elevating the head of the bed to around 30 degrees and by using iso-osmotic feeds.
Watch the Compat Soft video to learn more about NG tube placement and daily care.
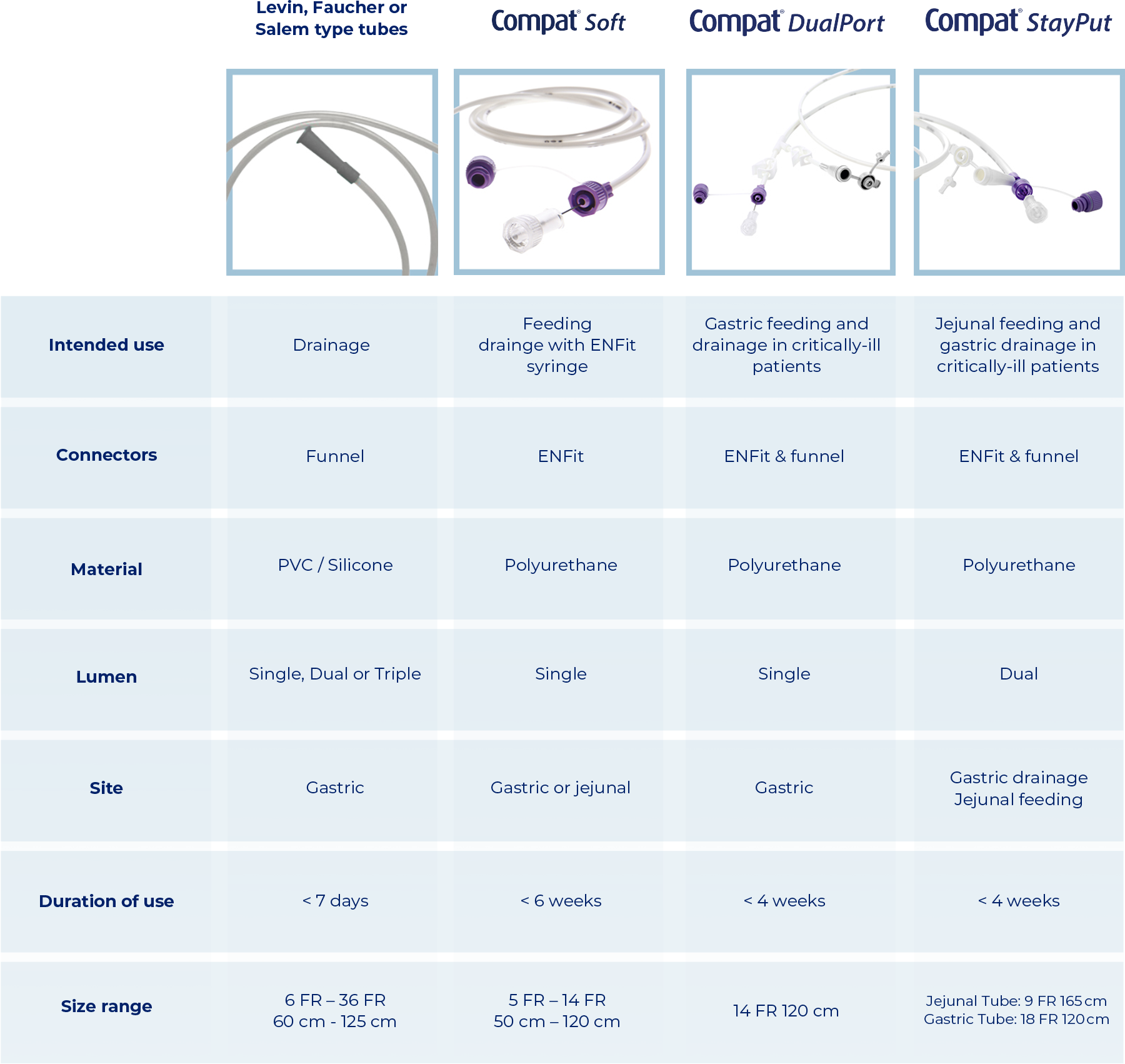
Overview of NGTs
Discover the Compat Nasogastric Feeding Tubes Range