Gastric Residual Volume – Monitoring and Management
An overview of critical care guidelines for enteral nutrition (EN) and the use of gastric residual volume (GRV) management and monitoring as an essential component of EN patient care to help prevent complications.
Malnutrition in Critically Ill and the Use of Enteral or Parenteral Nutrition
Disease-related malnutrition is a common problem among hospitalised patients. Specifically, in critically ill patients, oral food intake may not provide the required nutritional value. This may be due to the illness, nausea, vomiting, difficulty in swallowing and early satiety. Critically ill patients can have their oral intake also affected by mechanical ventilation, gastrointestinal surgery or unconsciousness (Yasuda et al. 2019).
In such patients, enteral nutrition (EN) or parenteral nutrition (PN) may be used to compensate for nutritional intake. Critical care guidelines recommend EN over PN in hospitalised patients who require non-oral nutrition therapy, except in cases where EN is contraindicated. EN is generally a riskless and well-tolerated approach in patients with normal gastrointestinal (GI) function.
Gastrointestinal Dysfunction and Gastric Residual Volume
GI dysfunction can be an obstacle to EN. Feeding intolerance is an important indicator of GI dysfunction and is caused by delayed gastric emptying. Gastric emptying is assessed in clinical practice by measuring the gastric residual volume (GRV), which is the amount of liquid drained from the stomach following EN. GRV is measured by aspiration using a syringe or gravity drainage to a reservoir (Elke et al. 2015).
GRV management and monitoring are essential components of EN patient care and can help prevent complications. GRV management can allow clinicians to identify patients with delayed gastric emptying earlier to implement strategies that would minimise the effects of feeding intolerance. As per the SCCM/ASPEN 2016 guidelines (McClave et al. 2016), patients should be monitored for tolerance of EN, and inappropriate cessation of EN should be avoided. Holding EN for GRV <500 mL in the absence of other signs of intolerance should be avoided. In addition, the time period that a patient is made nil per os (NPO) prior to, during, and immediately following the time of diagnostic tests or procedures should be minimised to prevent inadequate delivery of nutrients and prolonged periods of ileus. Ileus may be propagated by NPO status (ICU Enteral Feeding Guidelines 2012).
The limit for normal GRV was proposed as 200 mL for nasogastric feeding (McClave et al. 1992). While this recommendation has been used in clinical practice, the normal limit for GRV in critically ill patients treated with EN still varies from ICU to ICU. Values between 50 mL to 500 mL can be found in the literature (Montejo et al. 2010). The REGANE study showed that increasing the limit of monitored GRV from 200 to 500 mL did not increase pneumonia (Montejo et al. 2010), while findings from the NUTRIREA 1 clinical trial showed that adopting a no-routine monitoring of GRV approach did not increase pneumonia (Reignier et al. 2013). Both these studies included ICU patients. In another study, Chapman et al. (2009) showed that 24-hour GRV of greater than 250 mL was shown to predict slow gastric emptying, but sensitivity and the negative predictive value was modest.
Overall, ICUs around the world continue to monitor GRV with different frequency, ranging from 4 hours to every 24 hours. European guidelines recommend delaying EN if GRV is above 500 mL/6h and other international guidelines also recommend GRV monitoring in patients with feeding intolerance and/or risk of aspiration (Yasuda et al. 2019).
Enteral Access Medical Devices Designed to Ease GRV Management
Two Compat products are especially designed to ease GRV management in critically-ill patients.
-
Compat DualPort: single lumen dual port nasogastric tube.
It is designed to help simplify gastric drainage and enteral tube feeding through the use of one single tube for both operations. It is compatible with most drainage/suction devices and is designed to ease fluid flow. Its Y-tube design with clamps facilitates tube handling and helps prevent fluid leakage.
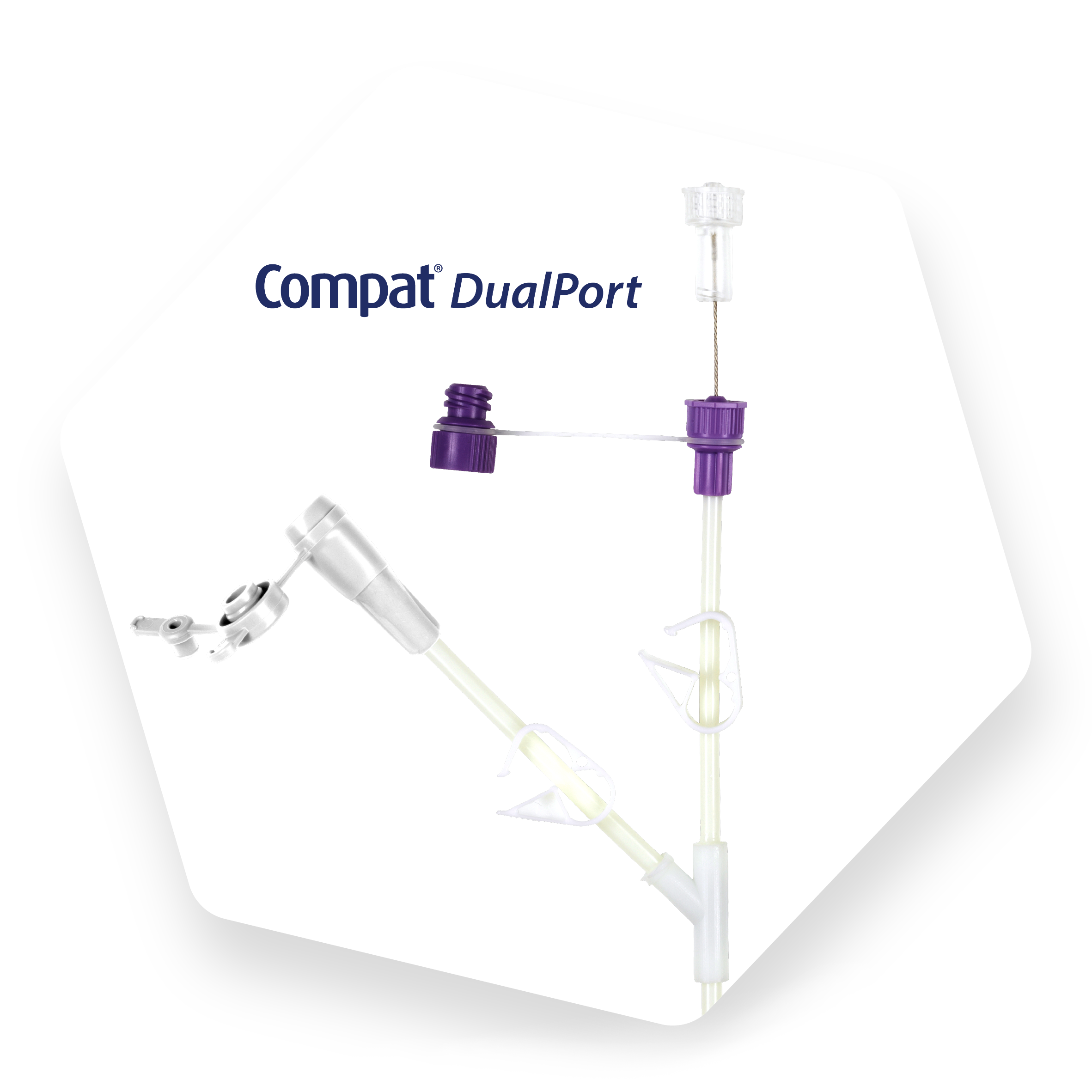
Discover how to use Compat DualPort for gastric feeding and drainage by watching the video.
-
Compat Modum: closed system gastric residuals aspiration and measurement accessory.
It is designed to ease GRV management as it enables closed system gastric residuals aspiration into a collection bag, reducing exposure to gastric fluids and the risk of contamination. It is compatible with most enteral tubes, syringes and drainage/suction devices.
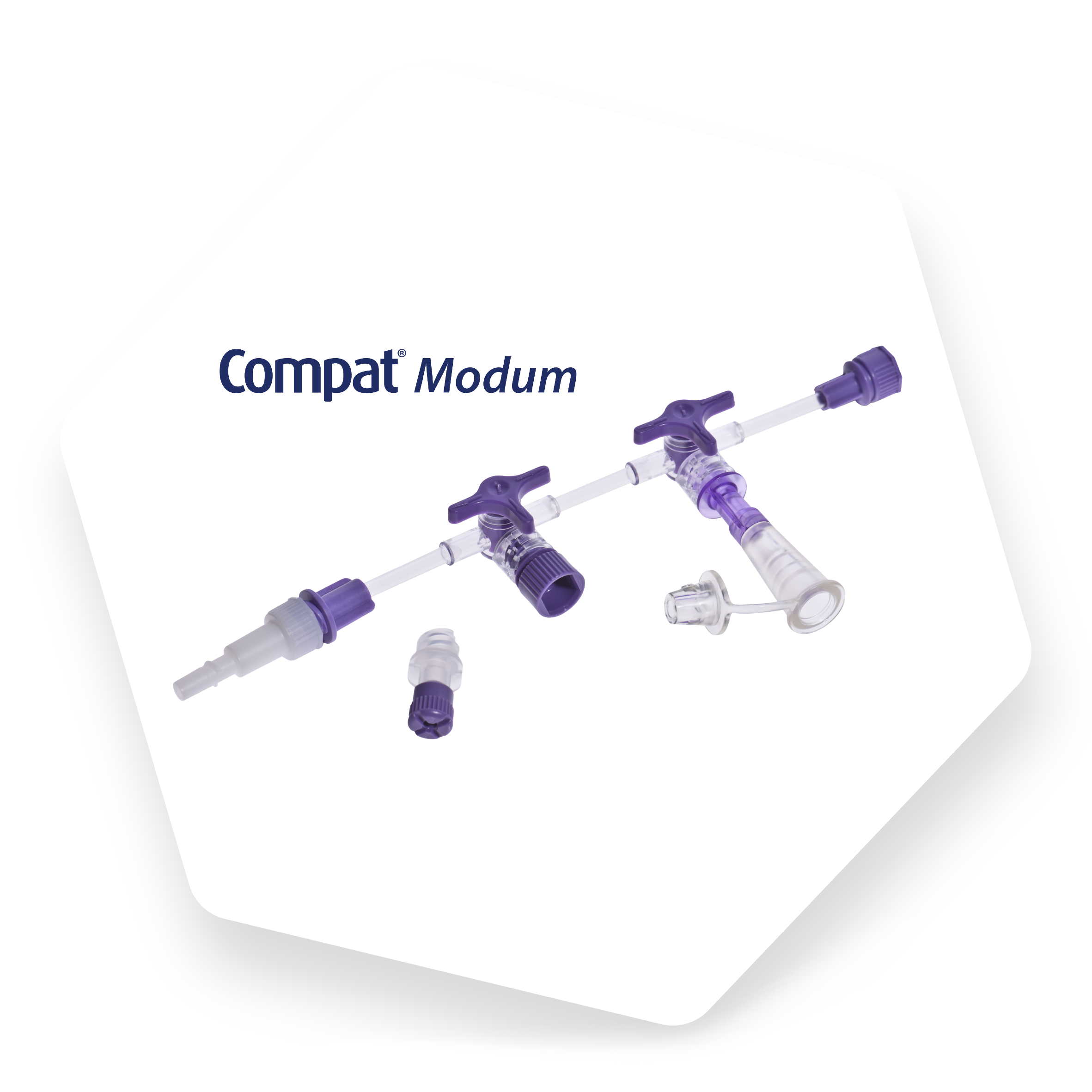
Watch this video to discover how to use Compat Modum for GRV aspiration and measurement.

